Case 3
Contributors
Dr. Ambika Gayad, Dr. Kiran
Radiological Findings, Disease course and Management
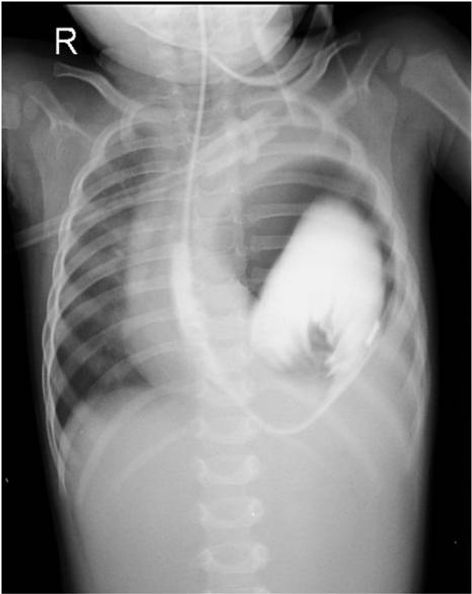
Initial Chest Radiograph
15 Sept 2015 14:34
-
Bowel loops in the left hemithorax with mediastinal shift towards right
-
Left hemidiaphragm not clearly visualized
Initial Diagnosis
Left diaphragmatic hernia/eventration
Repeat Chest Radiograph
16 September 2015 09:55 am
-
Stomach displaced into the thorax
-
Gross dilatation of stomach
-
Greater curvature directed superiorly and lesser curvature directed inferiorly
-
NG tube tip at the gastro-esophageal junction
Diagnosis
Diaphragmatic hernia/eventration with gastric volvulus
Contrast Study
Gastrografin swallow performed to confirm the diagnosis.
16 Sept 2015 12:39
-
Reflux of contrast back into the nasogastric tube after 40 ml of contrast was instilled, confirming the diagnosis of gastric volvulus.
Surgical Findings
Hypoplastic left lung
Small bowel, spleen and stomach seen in the thoracic cavity
Diaphragmatic defect seen measuring 5 x 4 x 3 cm.
Well developed anterior lip and hypoplastic posterior lip
Management
Diaphragmatic hernia repair with gastropexy
Contents placed in abdominal cavity
Defect closed
Intercostal Drainage Tube (ICDT) placed in left thoracic cavity
Post operative course
Chest Radiograph
Normal position of left diaphragm and mediastinum
Course in hospital
Course in the hospital was uneventful. The child is presently normal and has been advised follow up.
Discussion
-
The presence of a defect in the diaphragm increases the risk of gastric volvulus.
-
The stomach is fixed by four ligaments (gastrocolic, gastrohepatic, gastrophrenic and gastrosplenic ligaments)
-
Anomalies in these ligaments may increase the chance for the presence of a gastric volvulus.
-
Gastric fixation can be elongated or absent in patients with diaphragmatic defects (CDH, diaphragmatic eventration, hiatal hernia) as ligaments are normally inserted in the diaphragms
-
Predisposing factor for an abnormal stomach rotation.
-
Increased space under the diaphragmatic defect also increases the risk of gastric volvulus
Gastric volvulus is a rare clinical entity defined as an abnormal rotation of the stomach of more than 180°, creating a closed-loop obstruction that can result in incarceration and strangulation.Gastric volvulus in children is often secondary to congenital diaphragmatic defects.
Classification
Gastric volvulus, is frequently classified in relation to the axis around which the stomach rotates and includes the following three types
1. Organoaxial:
-
Stomach rotates around an axis that connects the gastroesophageal junction and the pylorus
-
Antrum rotates in opposite direction to the fundus of the stomach.
-
Most common type of gastric volvulus,usually associated with diaphragmatic defects
2. Mesenteroaxial
-
Mesenteroaxial axis bisects the lesser and greater curvatures.
-
Antrum rotates anteriorly and superiorly
-
The posterior surface of the stomach lies anteriorly
-
Rotation usually incomplete and occurs intermittently
-
Usually, present without diaphragmatic defects and usually have chronic symptoms
3. Combined
-
A rare form in which stomach twists both mesenteroaxially and organoaxially.
References
-
Perez-Egide, L., Parente, A., & Cerda, J. (2015, November 23). Acute gastric volvulus and congenital diaphragmatic hernia, case report and review. African journal of Paediatric Surgery.Retrieved January 26, 2016, from http://www.afrjpaedsurg.org/article.asp?issn=0189-6725;year =2015 ;volume =12; issue =3; spage=200;epage=202;aulast=P%E9rez-Egido
-
Hope, W. (2015, April 02). Gastric Volvulus. Medscape News and Perspective. Retrieved January 26, 2016, from http://emedicine. medscape.com/article/2054271-overview
Diagnosis
Left diaphragmatic hernia/eventration
Gastric volvulus organo-axial type
Hypoplastic left lung